
What is Cranial Osteopathy?
Because the craniosacral system encompasses the brain and spinal cord, it influences the entire nervous system, affecting many body functions. Patients often report a sense of deep relaxation during and after the cranial treatment session and may feel light-headed. These effects are popularly associated with increases in endorphins, but research shows they may be brought about by the endocannabinoid system.

Read More
Cranial osteopathy (aka Cranial Therapy or Cranial-Sacral Therapy) is based on the fact that the central nervous system, including the brain and spinal cord, has subtle, rhythmic pulsations that are vital to health and can be detected and modified by a skilled practitioner.
“Osteopathy in the Cranial Field has gained a special position within the many dimensions of osteopathic medicine. The underlying causes of severe pathological disturbances are to be found in cerebrovascular insufficiency and impaired cerebrospinal fluid circulation. Throughout the early development of osteopathic medicine, Dr. Andrew Taylor Still, its founder, paid special attention to the cerebrovascular and cerebrospinal systems. The role of these systems was well known to him at the end of the XIX Century. He appreciated their respective dominance in body physiology. Another enlightened pioneer, Dr. William G. Sutherland, who advanced osteopathy into the cranial field, recognized the significance of slow fluctuations arising within the cranium, which could be responsible for skull bone motion.”[1]
Dr. Sutherland defined this motion as the Primary Respiratory Mechanism in the 1930s. The PRM according to Sutherland “includes a number of structural or anatomical elements namely brain, blood vessels, meninges, the cranial bones with their delicate articular design of sutures and the reciprocal tension membrane of dura mater. Within the cranium there is the source of the special physical forces, which initiate the cranial rhythmic impulse and skull bone motion.”[2]
“Experimental and clinical observations demonstrate that relations between main parameters specific for CV (cerebrovascular) and CSF (cerebral spinal fluid) systems are complex. … For example, in one combination of primary factors, if arterial volume increases, cerebral blood flow (CBF) increases together with increase of intracranial pressure (ICP), but if venous volume inside the cranium increases or outflow of CSF to spinal cavity is obstructed, increase of ICP will be accompanied by a decrease of CBF.”[3]
Hence, osteopathic manual therapy to skull bones that encourages appropriate, balanced CSF flow (assessed through the cranial rhythmic impulse at 8-12 cycles/min) allows for the proper CBF (arterial and venous), normal ICP, and overall oxygenation and nourishment of the brain.
[1] Moskalenko, Y., Frymann, V., Kravchenko, T., & Weinstein, G. (2003). Physiological Background of the Cranial Rhythmic Impulse and The Primary Respiratory Mechanism. The AAO Journal, 2003, V.13, No.2, P.21-33
[2] Ibid
[3] Ibid.
Benefits of Cranial Osteopathy
- Improved and balanced cerebral spinal fluid (CSF) flow
- Allows for proper CBF (arterial and venous), normal ICP, and overall oxygenation and nourishment of the brain
- Reduces headache pain
- Increases nourishment of brain tissue
The practice of osteopathic medicine has been in use since 1874. Many studies have shown that the manipulation from cranial osteopathy reduces pain, sleep disturbance, anxiety, and all around improved quality of life. After just two weeks of cranial osteopathy, TBI survivors found a decrease in headaches, vertigo, muscle tension, and an improvement in their general well-being.
How Cranial Osteopathy Works
With cranial osteopathy, a craniosacral practitioner uses gentle hands to knead the 22 cranial bones, membranes, and CSF. This cranial manipulation addresses areas of restricted movement that compromise function to re-establish normal movement, subsequently reducing pain and improving daily functioning.
Because the craniosacral system encompasses the brain and spinal cord, it influences the entire nervous system, affecting many body functions. Patients often report a sense of deep relaxation during and after the cranial treatment session, and may feel light-headed. These effects are popularly associated with increases in endorphins, but research shows they may actually be brought about by the endocannabinoid system.
Cranial Osteopathy for TBI
For TBI patients, it is key to gauge the therapy per the patient. Ideally, a patient should get no more than one 30 to 60-minute cranial session per week. “Touch up” cranial therapy treatments may be done for 15-20 minutes that same week or done after another associated procedure, such as nasal specific or intranasal PRP.
It is postulated that head pain may frequently arise from or be influenced by various soft tissues and neurogenic or osseous structures of the head, neck, and upper body. Pain elicits a heightened response of the sympathetic nervous system that can create a vicious cycle by causing vasoconstriction, ischemia, chemical changes, more muscle contraction, and thus, more pain.
Techniques of cranial osteopathy are believed to improve circulation; release restrictions in joints; reduce tension in the muscles, fascia, and dura mater; decrease nociceptive input; and promote the normalization or calming of the central nervous system in traumatic brain injury (TBI) patients.*
*Results may vary; no guarantee of specific results
Prior literature has emphasized the importance of focusing on the occipitoatlantal joint, occipital condyles, and occipitomastoid joint; sphenobasilar syncondrosis in migraine; and use of craniosacral techniques for cervicogenic headache. In at least one small case series, cranial osteopathy was shown to be a helpful adjunctive therapy to traditional pharmacologic therapies for U.S. soldiers suffering from posttraumatic headache attributed to mild head injury.

Read More
Regional brain blood supply is determined not only by hemodynamic factors but also by CSF mobility. Therefore, if resistivity of CSF pathways increases, the regional CBF will decrease, and this may be the explanation of some kinds of neurological deficit. Such a situation might be one of the consequences of brain injury. In this case the appropriate osteopathic techniques could increase the CSF circulation in the injured brain region.
Numerous experiments have determined that “slow fluctuation of cerebral blood flow closely correlate with local fluctuations of brain blood volume and oxygen availability in brain tissue.” Recent applications of spectral analysis have shown (Moskalenko 2000, Moskalenko et al. 2001) that slow fluctuations are composed of extracranial fluctuations of arterial pressure and respiratory chest movements, and of intracranial fluctuations namely redistribution of CSF volumes inside skull.
One key experiment has been to measure how CSF and CV flow during a single cardiac cycle using 2 different parameters. The most acceptable test is a “combination of simultaneous recordings of Bio-Impedance (B-Imp) and transcranial dopplerography (TCD), because these methods are based on different physical principles and, therefore, reflect different aspects of the functioning of CV and CSF systems. Indeed, B-Imp records the change of electrical conductivity between plate electrodes, placed on the human head, for high frequency (50-70 kHz) electrical current. Because electrical conductivity of blood and CSF are different (for blood it is about half that for CSF), their comparative volume changes will change the electrical conductivity between electrodes.”[1]
The following figure compares the CSF flow (represented by t) of a healthy person, an athlete, and a TBI patient. It was found that “t”, translated as “CSF mobility” was greatest in the athlete, normal in the healthy person, and significantly smaller in the TBI patient. In very simplistic terms, if we think of the CSF as an abundant river of fluid circulating the brain and spinal column, that river is stagnant and restricted in the TBI patient. See Figure 5.
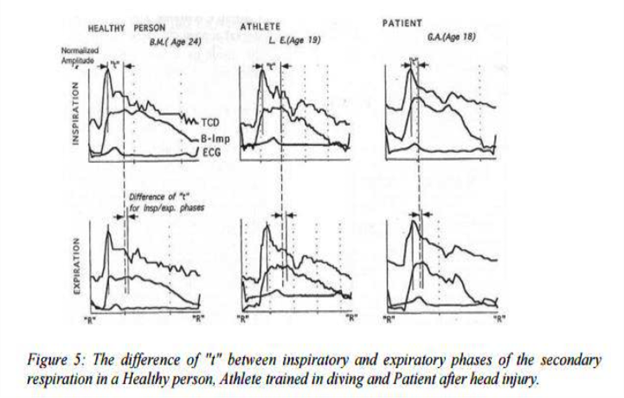
Time shift between peaks of TCD and В-Imp is determined by the replacement of some portion of CSF out from (or into) zone of В-Imp electrodes. Thus, this time interval represents the mobility оf CSF inside the cranium during the pulse cycle. At this period no active processes could operate. Investigations under different conditions have shown that “t” reflects CSF mobility.
In sum, CSF motility (along with CV flow), can be assessed and addressed by the osteopathic practitioner via the CRI. The CRI can be felt as the subtle motion of the skull bones. Encouraging an improved CRI by the cranial osteopathic practitioner is a significant way to positively affect the primary respiratory mechanism and overall metabolic and neurovascular health of the brain.
[1] Ibid.
Safety and Side Effects
Cranial osteopathy, while a subtle therapy, should not be taken lightly. Due to the increasing popularity of massage and other manual therapies, it is very easy for a lay practitioner to learn a few cranial techniques that manipulate the skull but fail to acknowledge the key purpose of syncing these techniques with the CRI as well as the limits of each patient. Hence, while cranial osteopathy, if done poorly, has only a benign, transient effect on the patient, it may be that the patient experiences increased head pressure, headache pain, or emotional distress due to the therapy. All practitioners, whether trained as osteopathic physicians or not, must work to be careful with the treatment, always assessing the CRI as his or her guide for more or less therapy to any particular area of the skull.