Call for a consultation 970-927-0466
info@tbitherapy.com
Facebook
X
Facebook
X
Home
About
Our Team
Our Partners
Testing for TBI
Packages and Payment
Welcome Packet
Treatments
HBOT
Intranasal Insulin
Intranasal Bioactive Plasma
Intranasal RPC
Cellular Nutrition
Cranial Osteopathy
Peptide Therapy
Adjunctive Therapies
Testimonials
Resources
Personal Injury Resouces
Scientific References
Recent Posts
PowerPoint Lectures
Videos and Podcasts
Webinars
Supplements
Designs for Health
Elk Antler
Extreme Hydration
TBI Intro Pack
Ultimate Detox
Contact & Location
Schedule
Select Page
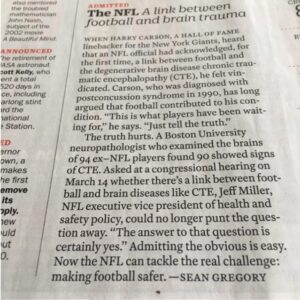
Time Magazine
Recent Posts
Microplastics and Dementia
The Effect of Intranasal Plus Transcranial Photobiomodulation on TBI
Electrophysiological trajectories of concussion recovery: From acute to prolonged stages in late teenagers
Former Navy SEAL, FBI agent brings leadership training to Roaring Fork Valley
The Longevity Project: Experts discuss brain health and injuries
We use cookies to ensure that we give you the best experience on our website. If you continue to use this site we will assume that you are happy with it.
Ok